Emetophobia Treatment
Fear of Vomiting
What is Emetophobia?
Emetophobia, or the fear of vomiting, is among the least studied phobias despite it being not a rare condition.
If you are suffering from this condition, it can be a lonely experience, as it is likely that you know of no one else personally who has to deal with what you have to deal with. This guide is designed to help you get as educated as possible about Emetophobia. If you then feel you are ready to tackle this with our evidence based program, you can purchase it here.
This information guide gives you a lot of background information about Emetophobia including how do we assess if you meet criteria for Emetophobia, the different treatment models in the scientific literature, and how to make sure that you really suffer from Emetophobia and not another condition that can seem similar. We even discuss the physiological aspects of nausea and vomiting itself.
Introduction
Compared to other specific phobias, phobias of vomiting are more likely to be strongly associated with a high level of anxiety over specific physical sensations especially that can link to the feeling that person may vomit.
These fears of physical sensations can arise in any location and can include nausea, tightness in the throat and other uncomfortable feelings. Ironically, people with Emetophobia are often hypervigilant to their physical sensations with increases their awareness of slight changes in their physiology which can then maintain their anxiety in a feedback loop. Research has indicated that Emetophobia may be more debilitating than other well know phobias such as spiders and heights (Kartsounis, Mervyn-Smith, and Pickersgill ,1983).
The Diagnostic and Statistical Manual of Mental Disorders 5th edition, specifies Emetophobia as a Specific Phobia: Other Type: Vomiting. Prevalance estimates range from 1.7% to 3.1% for males and from 6% to 7% for females (Philips, 1985; van Hout & Bouman, 2006).
Research has uncovered that the usual age of onset occurs between late childhood and adolescence (7.5 to 15.7 years of age). The average length of time someone will suffer from this phobia once they have it, and it is untreated, has been estimated at 25.9 years.
Of people diagnosed with Emetophobia, the rate of fear of self-vomiting has been shown to be approximately 47%, fear of others vomiting to be around 13% and for an equal fear of both approximately 36%. It has been hypothesised that the fear of others vomiting may be related to the possibility of contagion leading to the person ending up vomiting themselves.
Research has shown a number of fears related to vomit/vomiting for people with Emetophobia:
| ● Getting contaminated and becoming ill | 50.5% |
| ● Fear of nausea and vomiting | 100% |
| ● Fear of a heart attack | 30.4% |
| ● Fear of panic | 29.4% |
| ● Fear of losing control | 19.1% |
| ● The features of vomit: | |
| ○ Sight | 72% |
| ○ Sound | 71 % |
| ○ Taste | 4.8% |
| ○ Smell | 66% |
| ● Suffocation | 37.3% |
| ● Gagging | 83.8% |
Life Impact
As body sensations such as gastrointestinal complaints or nausea can occur on a daily basis the degree of interference can be higher than for other phobias which can be more easily avoided. Those with Emetophobia report nausea almost every day especially when anxious. Interestingly, nausea is not linked to actual experiences of vomiting. This may be at least partially explained by the appraisal of nausea as a signal of impending threat (vomiting) which leads to anxiety and behaviours to reduce the likelihood of vomiting occurring.
Triggers
There can be both external and internal triggers in Emetophobia. Listed below are some common ones and where research exists about the prevalence this has been included as a % of people with Emetophobia who this relates to.
External Triggers
Avoidance of certain categories of people
| ● Children or adults who may be sick (and contagious) | 80.9% |
| ● People at risk of vomiting (e.g. people who are drunk) | 85.9% |
Avoidance of certain situations
| ● Going on an overseas holiday or visiting foreign countries | 71.1% |
| ● Anywhere where drunk people may be | 85.9% |
| ● Crowded places | 65.1% |
| ● Traveling by boat | 89.3% |
| ● Traveling by plane | 68.7% |
| ● Drinking alcohol | 65.6% |
| ● Illegal substances | 92.3% |
| ● Being in crowds with alcohol | 62% |
| ● Fairground rides | 86.9% |
| ● Public transport | 64.4% |
| ● Going to new places | 70% |
| ● Skipping classes | 9% |
| ● Having to leave work frequently | 19.6% |
| ● Becoming pregnant | 5.3% |
| ● Visiting others in hospital | 56.8% |
| ● Using public toilets | 51.5% |
| ● Being left alone with young children | 34% |
| ● Taking medication | |
| ● Going to the dentist |
Avoidance of food
| ● Minimising the amount of food in one’s stomach to reduce the amount that could be potentially vomited. | |
| ● Minimising food in certain contexts such as restaurants or anything cooked by someone else | |
| ○ Salad bars or buffets | 54.1% |
| ○ Restaurants | 55.7% |
| ● Avoiding or restricting certain types of foods: (e.g. dairy, fast food, shellfish) | |
| ○ Seafood and Shellfish | 65.7% |
| ○ Meat | 45.6% |
| ○ Fish | 14.9% |
| ○ Dairy | 17.6% |
| ○ Eggs | 22.3% |
| ○ Fruits and Vegetables | 24% |
| ○ Fried fast food | 21% |
| ○ Bread, pastry and cakes | 18% |
| ● Avoiding foods that were linked with previous episodes of vomiting | |
| ● Just eating a narrow range of food considered “safe” | |
Internal Triggers
| ● Avoidance of thoughts and images related to vomiting. This may be seen by using alternative words and phrases than vomiting. Being unwell or being ill are two examples. Distraction, suppression of thoughts are common methods to attempts to prevent thoughts about vomiting. |
| ● Avoidance of gastrointestinal symptoms and nausea. This can include restricting the amount and type of food and drink consumed to minimise any gastrointestinal symptoms. |
Safety Behaviours
Safety behaviours can be employed when someone with Emetophobia is unable to escape or avoid what they feel is a risky situation. Safety behaviours can be overt and observable or covert and private.
An overt behaviour would be constantly checking “use by” dates, excessive cooking of food or excessive cleaning of the kitchen. Taking anti-nausea medication, antacids, or mints would also fit into this category.
A covert safety behaviour example could be repeating a word a number of times to attempt to prevent vomiting.
Research has uncovered many common safety behaviours people with Emetophobia engage with:
| ● Checking expiry dates on food regularly | 64.9% |
| ● Washing hands excessively | 42.1% |
| ● Checking the state of own health excessively | 80.8% |
| ● Checking the state of other’s health excessively | 44.9% |
| ● Avoiding anaesthesia or surgery | 34% |
| ● Overcooking their food | 62.4% |
| ● Engaging in eating rituals | 52.7% |
| ● Reassured themselves | 52.7% |
| ● Seek reassurance from others | 30% |
Assessment for Emetophobia
The most common cognitive processes in Emetophobia are worry and mentally planning how to prevent oneself from getting sick or how to cope if someone in their presence is sick. People often have beliefs about the value of worrying related to a phobia of vomiting. Two common beliefs are “If I worry I can prevent vomiting from happening” and “If I worry I can mentally prepare myself for vomiting.” These types of beliefs are often examined in an evidence based treatment program.
Currently there are two empirically validated measures to test for the presence of Emetophobia.
The SPOVI is a 14 item self-report measure that focuses on cognitive processes, safety seeking and avoidance behaviours over the last week. Each item is rated on a scale from 0 (not at all) to 4 (all the time). Scores can range from 0 to 56. SPOVI items can be divided into two subscales: avoidance and monitoring of threat.
SPOVI
The SPOVI is a 14 item self-report measure that focuses on cognitive processes, safety seeking and avoidance behaviours over the last week. Each item is rated on a scale from 0 (not at all) to 4 (all the time). Scores can range from 0 to 56. SPOVI items can be divided into two subscales: avoidance and monitoring of threat.
The SPOVI has been shown to be sensitive to treatment change and has been shown to be useful as a session by session monitoring tool in therapy.
An optimal clinical cut-off score for the SPOVI when investigating the presence of Emetophobia has been determined in the research to be 10.
A link to the SPOVI can be found here.
EmetQ-13
The EmetQ-13 has a range of 13-65 with an appropriate cut off score of 22 to determine the presence of a specific phobia of vomiting (SPOV).
The EmetQ and SPOVI overlap in assessing some emetophobia symptoms. The EmetQ is less sensitive to change than the SPOVI. Part of the explanation is that the SPOVI is more focused on processes involved in change and therefore more likely to be reflected in SPOVI scores.
The EmetQ and SPOVI overlap on assessing avoidance but the EmetQ separates avoidance into two distinct categories: avoidance of situations and movement, and avoidance of people who may vomit.
The EmetQ also includes another factor related to the misinterpretation of seeing or smelling vomit in anticipation of vomiting by oneself.
The SPOVI also contains items that assess an individuals monitoring of the threat of vomiting (eg excessive worry).
Thus, the two measures have slightly different emphases in their assessment of Emetophobia.
A link to the EmetQ-13 can be found here.
Treatment Models

Treatment models are often used to try to make sense of all the factors that are relevant in the understanding and treatment of a condition. These models can range in complexity from the very simple that just summarise very general features to the very complex that try to incorporate as many variables as possible.
For the sake of completeness we will discuss 4 models in increasing order of complexity.
Model 1:
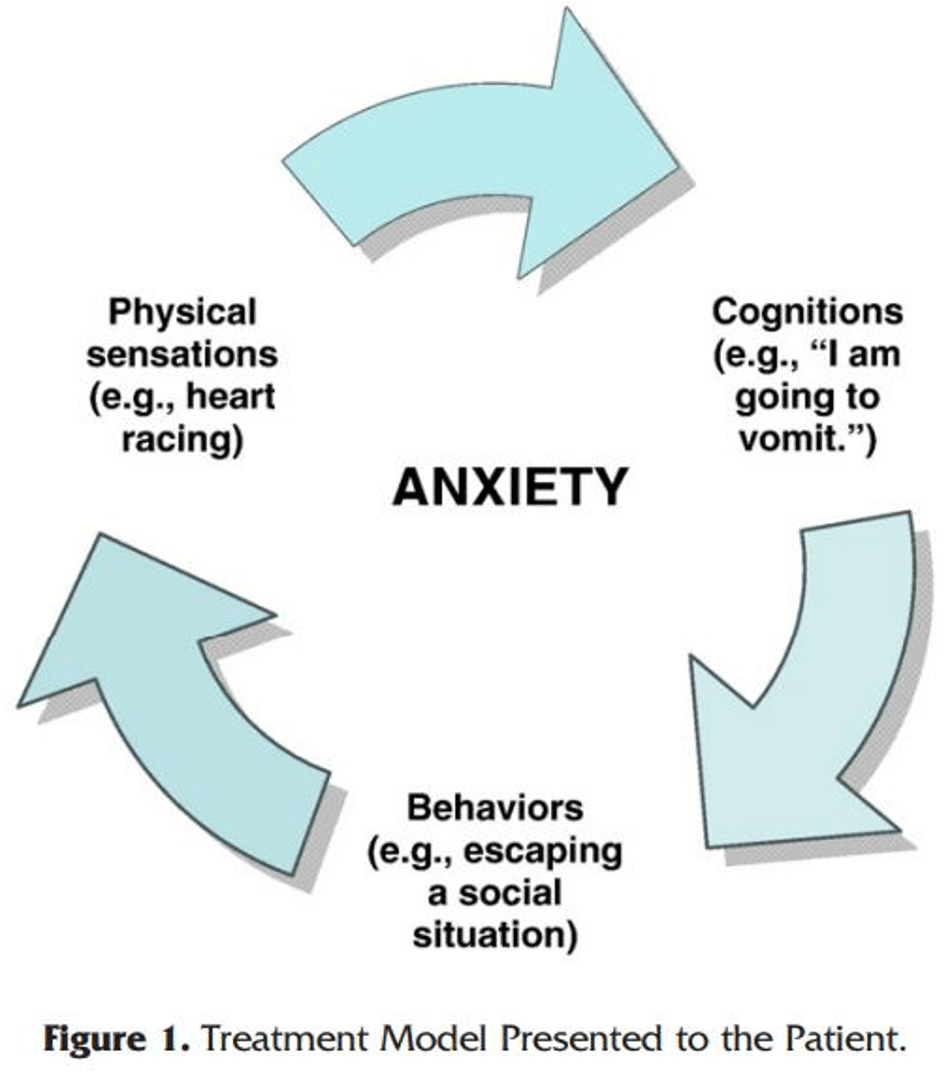
Model 1 is our simplest example of a model. It shows the circularity of the processes that maintain emetophobia.
Model 2:
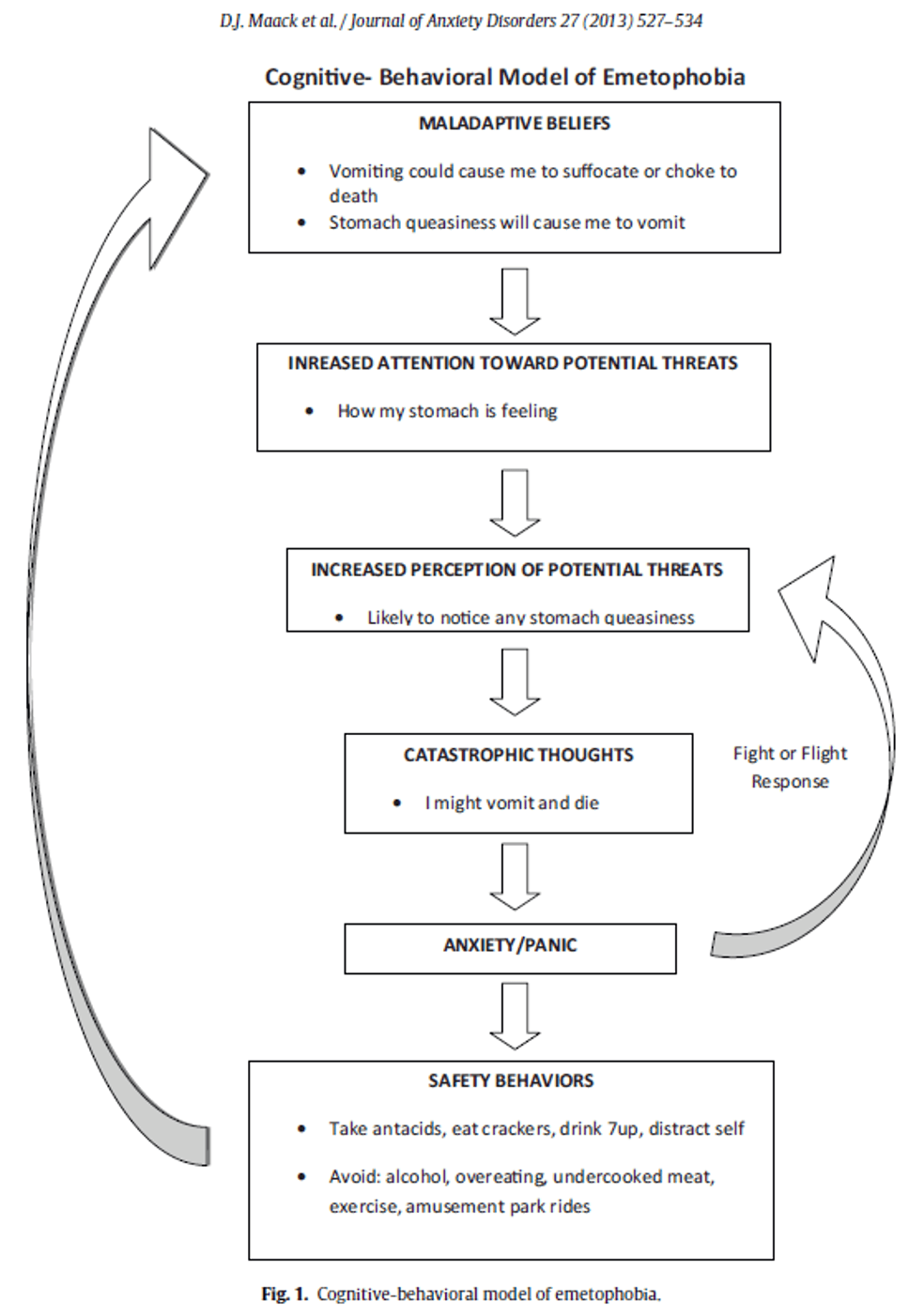
Model 2 is a more sophisticated version of Model 1. As can be seen it is a more detailed description of the relevant processes. The higher level of details makes it more clear to a clinician what treatment targets should be and how to construct processes and techniques to target them.
Models 3 and 4 are the most sophisticated and have multi-dimensional components. They thus require some work to understand their mechanisms.
Model 3:
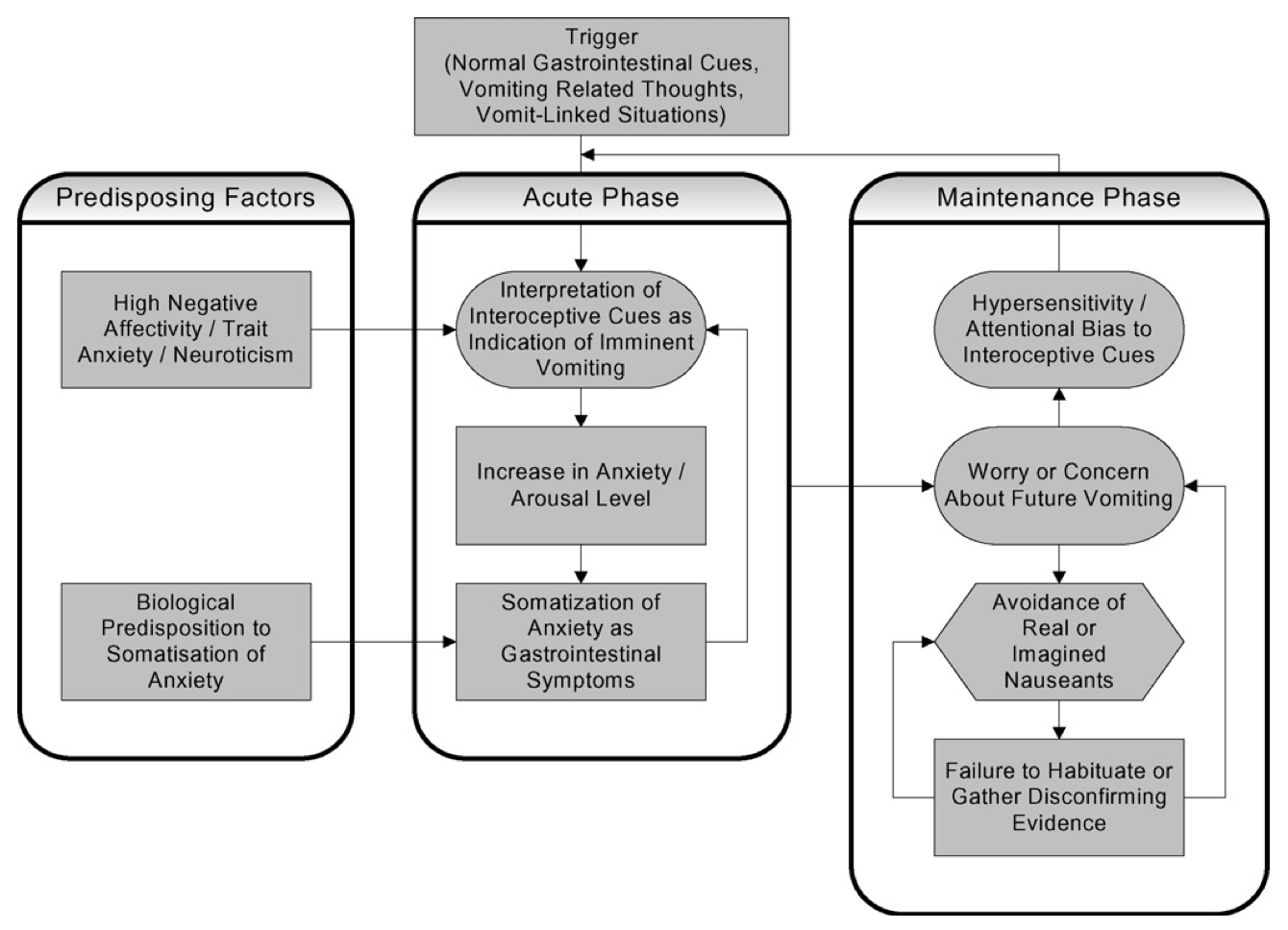
This model, Boschen (2007) breaks down the components of Emetophobia into 3 major areas:
- Predisposing Factors
- Acute Phase
- Maintenance Phase
He argues that two major factors influence and increase the risk of someone developing emetophobia. The first is their base level of general background anxiety and second the second is their tendency to express their anxiety through physical symptoms such as “butterflies”.
Model 4:
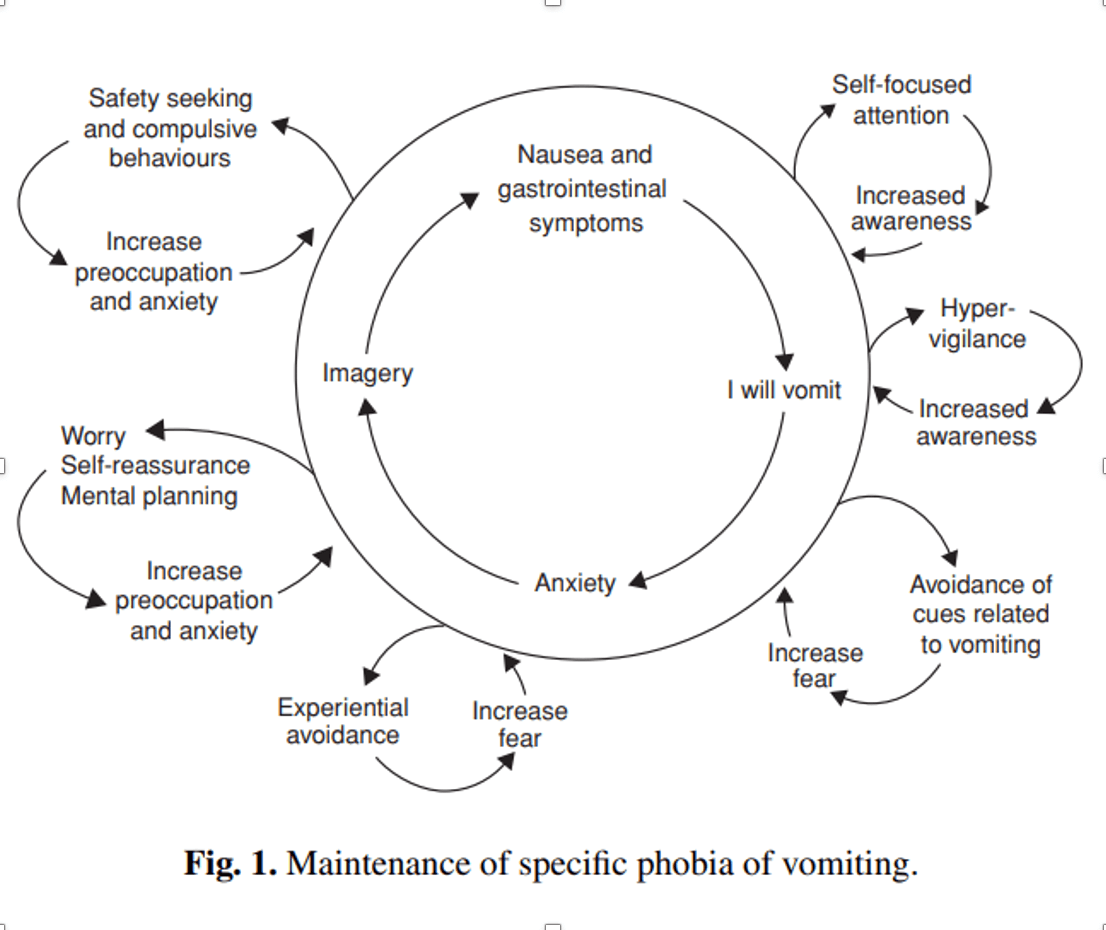
Veale’s model (Model 4) has aversive memories of vomiting as a current driver of a fear of vomiting as a central tenet. Past negative memories of oneself vomiting become linked with the present so that they are experienced as if they are just about to be repeated.
Once a trigger has occurred a number of responses tend to arise automatically that are attempts to manage the fear of vomiting but actually contribute to its maintenance:
- Avoidance of thoughts and images of oneself or others vomiting.
- Avoidance of cues that may increase the feeling of nausea.
- High intensity monitoring for external threats (eg a sick child).
- High intensity monitoring of internal body sensations and the appearance of nausea symptoms.
- Ongoing worry and responses to worry such as self-reassurance and mental planning.
- A belief that one can stop oneself from vomiting with the “right strategies” as well as an over-inflated sense of responsibility for doing so.
- Safety behaviours that may include compulsive checking and reassurance seeking.
All of these strategies prevent the disconfirmation of expectations, even in the face of low incidence of actual vomiting occurring. In fact, it is often assumed that these factors are actually preventing episodes of vomiting and are therefore reinforced in a form of a feedback loop.
To understand this in more simple terms we can refer to an old joke. A person sees their neighbour wearing garlic around their neck. He asks his neighbour:
“Why are you wearing garlic around your neck?”
The neighbour replies:
“To keep the vampires away”
To which the person responds:
“But there aren’t any vampires!”
The neighbour replies
“Exactly! That’s why I need to keep wearing the garlic around my neck so they don’t come back!
Co-occurring Disorders
| ● Generalised Anxiety Disorder | 14.1% |
| ● Major Depressive Disorder | 13.6% |
| ● Panic Disorder | 10.2% |
| ● Social Phobia | 10.1% |
| ● Obsessive Compulsive Disorder | 9.6% |
| ● Agoraphobia | 5.5% |
| ● Health Anxiety | 2.8% |
| ● Eating Disorder | 1.4% |
It has been estimated that those diagnosed with Emetophobia will also have another diagnoseable disorder 27.7% of the time and 15.9% of those with Emetophobia will have at least two other diagnoseable disorders.
Emetophobia can appear on the surface similar to other disorders and therefore there is a high risk of misdiagnosis.
Differential Diagnosis
Let’s look at some of the disorders that can be mistakenly diagnosed instead of Emetophobia. It should be noted that it is possible for these disorders to occur in conjunction with Emetophobia.
Health Anxiety
People with Health Anxiety have a fear of being ill. Which illness the person thinks they may have can vary over time. Thus, their fear is of an illness rather than just vomiting per se. People with Emetophobia often have high levels of health anxiety in that they may worry about things like food poisoning or being infected which may lead them to vomit. Also, they may be more likely to attribute the cause of their nausea to a physical health condition rather than anxiety.
To legitimately receive a diagnosis of health anxiety above and beyond one of Emetophobia the person would have additional fears of illness that were unrelated to the fear of vomiting.
Obsessive-Compulsive Disorder
Those with Emetophobia often perform behaviours of a ritualistic nature to try to prevent vomiting and these behaviours usually begin after Emetophobia develops.
To legitimately receive a diagnosis of Obsessive Compulsive Disorder there would need to be additional obsessions and compulsions apparent that are not related to the attempt to prevent vomiting exclusively.
Panic Disorder
To receive a panic disorder diagnosis unexpected panic attacks need to be occurring with marked fear about the occurrence of future panic attacks. Sometimes the main fear of panic disorder is of vomiting when feeling nauseous and anxious. It is still possible to have additional spontaneous panic attacks that are not related to a fear of vomiting.
Social Phobia
The majority of people with Emetophobia fear vomiting whether they are alone or in social situations. People who predominantly fear negative judgement of others (and are not especially fearful of vomiting when they are alone) would potentially meet criteria for a diagnosis of social phobia.
Anorexia Nervosa
People with Emetophobia who are also underweight may be misdiagnosed with having anorexia nervosa. Additional information is required such as the extent to which food consumption is restricted and the reason food consumption is restricted.
With someone suffering from Emetophobia the aim of food restriction would be part of an attempt to eliminate the risk of vomiting (either totally or partially). These people do not actually want to be underweight, it is rather an unintended by-product of the attempt to remove risk of vomiting. This is not to say that this response to Emetophobia cannot evolve into an eating disorder in time.
It is extremely important to not misdiagnose someone with Emetophobia with an eating disorder as they are unlikely to identify with an eating disorder treatment model and will be left with little possibility of progress with a treatment plan built on that model.
There is often an overlap between Emetophobia, Panic Disorder, OCD and Social Anxiety Disorder. An individual with Emetophobia may have a fear of negative evaluation from others if they are sick, and therefore may present with symptoms similar to those found in Social Anxiety Disorder. Being preoccupied with gastrointestinal conditions and checking food ingredients and labels may happen in both Emetophobia and OCD. The symptoms of panic that can be experienced with Emetophobia can present as identical as the symptoms apparent in Panic Disorder.
Types of Therapies for Emetophobia
The most common evidence-based treatments for Emetophobia are exposure based therapies. Other types of therapeutic interventions have been reported in the literature including hypnosis, motivational techniques, psychodynamic therapy, contingency management, and psychotropic medication. However, these have lower levels of evidence for their efficacy and often involve a lot of time and effort for very little long term gains.
Emetophobia treatment has much higher dropout rates than other phobias in the literature, partly because of client’s strong fear of the prospect of vomiting as part of treatment. At the phobia solution we use are proprietary Find a Five technique which we have found is substantial upgrade to traditional exposure in Cognitive and Behavioural therapies and helps clients feel a much greater sense of control in treatment.
Nausea
As nausea is a significant focus for most Emetophobia sufferers a brief discussion about this phenomenon is warranted. Nausea is a difficult concept to define, evidenced by over 30 different definitions of the concept in the research literature. In fact, someone experiencing nausea often has difficulty defining their experience clearly. Variations of an unpleasant feeling that precedes vomiting is often a short hand answer.
Some people report the feeling in the stomach, others in the small bowel or colon and still others point to the esophagus as the centre of the nausea experience. Its often accompanied by other physical and psychological components such as fatigue, depression and anxiety.
What is the purpose of nausea?
We could say that nausea is a potential warning signal that there are internal or externally related dangers possibly occurring. Internally related signals could relate to a warming about possible damage or dysfunction in the digestive system to signal correct attention and action.
Externally related dangers could be a harmful or poisoned food. Sights, smells and tastes may evoke the warning sign through the experience of disgust. This disgust and our automatic reaction to it provided potential protection against ingesting something toxic.
Nausea can also be activated through behaviours related to movement and balance (eg motion sickness). The stomach is the key organ in the physiology of nausea in relation to motion sickness.
The specific mechanism that drives nausea is often unknown and the physiology of nausea is still poorly understood.
Phobia Solution
Our program has been over a decade in the making. We have used the best evidence-based components as well as made our own proprietary tweaks to enhance the experience of therapy especially our self-guided programs.
If you would like to purchase our program and work to put your phobia of vomiting behind you the link is here.
References
Ahlen, J., Edberg, E., Di Schiena, M., & Bergström, J. (2015). Cognitive behavioural group therapy for emetophobia: An open study in a psychiatric setting. Clinical Psychologist, 19(2), 96-104.
Bogusch, L. M., Moeller, M. T., & O’Brien, W. H. (2018). Case study of acceptance and commitment therapy and functional analysis for emetophobia. Clinical Case Studies, 17(2), 77-90.
Boschen, M. J. (2007). Reconceptualizing emetophobia: A cognitive–behavioral formulation and research agenda. Journal of anxiety disorders, 21(3), 407-419.
Boschen, M. J., Veale, D., Ellison, N., & Reddell, T. (2013). The Emetophobia Questionnaire (EmetQ-13): Psychometric validation of a measure of specific phobia of vomiting (Emetophobia). Journal of Anxiety Disorders, 27(7), 670-677.
Dargis, M., & Burk, L. (2019). A transdiagnostic approach to the treatment of emetophobia: A single case study. Clinical Case Studies, 18(1), 69-82.
Fix, R. L., Proctor, K. B., & Gray, W. N. (2016). Treating emetophobia and panic symptoms in an adolescent female: A case study. Clinical Case Studies, 15(4), 326-338.
Hunter, P. V., & Antony, M. M. (2009). Cognitive-behavioral treatment of emetophobia: The role of interoceptive exposure. Cognitive and Behavioral Practice, 16(1), 84-91.
Kannappan, A., & Middleman, A. B. (2020). Emetophobia: A case of nausea leading to dehydration in an adolescent female. SAGE Open Medical Case Reports, 8, 2050313X20951335.
Keyes, A., Deale, A., Foster, C., & Veale, D. (2020). Time intensive cognitive behavioural therapy for a specific phobia of vomiting: A single case experimental design. Journal of behavior therapy and experimental psychiatry, 66, 101523.
Keyes, A., Gilpin, H. R., & Veale, D. (2018). Phenomenology, epidemiology, co-morbidity and treatment of a specific phobia of vomiting: A systematic review of an understudied disorder. Clinical Psychology Review, 60, 15-31.
Klonoff, E. A., Knell, S. M., & Janata, J. W. (1984). Fear of nausea and vomiting: the interaction among psychosocial stressors, development transitions, and adventitious reinforcement. Journal of Clinical Child & Adolescent Psychology, 13(3), 263-267.
Kobori, O. (2011). Cognitive therapy for vomit phobia: A case report. Asia Pacific Journal of Counselling and Psychotherapy, 2(2), 171-178.
Lipsitz, J. D., Fyer, A. J., Paterniti, A., & Klein, D. F. (2001). Emetophobia: Preliminary results of an Internet survey. Depression and Anxiety, 14(2), 149-152.
Maack, D. J., Deacon, B. J., & Zhao, M. (2013). Exposure therapy for emetophobia: A case study with three-year follow-up. Journal of Anxiety Disorders, 27(5), 527-534.
Maack, D. J., Ebesutani, C., & Smitherman, T. A. (2018). Psychometric investigation of the specific phobia of vomiting inventory: A new factor model. International journal of methods in psychiatric research, 27(1), e1574.
Paulus, D. J., & Norton, P. J. (2016). Purging anxiety: A case study of transdignostic CBT for a complex fear of vomiting (emetophobia). Cognitive and Behavioral Practice, 23(2), 230-238.
Price, K., Veale, D., & Brewin, C. R. (2012). Intrusive imagery in people with a specific phobia of vomiting. Journal of behavior therapy and experimental psychiatry, 43(1), 672-678.
Riddle-Walker, L., Veale, D., Chapman, C., Ogle, F., Rosko, D., Najmi, S., … & Hicks, T. (2016). Cognitive behaviour therapy for specific phobia of vomiting (Emetophobia): A pilot randomized controlled trial. Journal of anxiety disorders, 43, 14-22.
Sykes, M., Boschen, M. J., & Conlon, E. G. (2016). Comorbidity in emetophobia (specific phobia of vomiting). Clinical psychology & psychotherapy, 23(4), 363-367.
van Hout, W. J., & Bouman, T. K. (2012). Clinical features, prevalence and psychiatric complaints in subjects with fear of vomiting. Clinical psychology & psychotherapy, 19(6), 531-539.
van Overveld, M., de Jong, P. J., Peters, M. L., van Hout, W. J., & Bouman, T. K. (2008). An internet-based study on the relation between disgust sensitivity and emetophobia. Journal of anxiety disorders, 22(3), 524-531.
Veale, D. (2009). Cognitive behaviour therapy for a specific phobia of vomiting. Cognitive Behaviour Therapist, 2(4).
Veale, D., & Lambrou, C. (2006). The psychopathology of vomit phobia. Behavioural and Cognitive Psychotherapy, 34(2), 139.
Veale, D., Ellison, N., Boschen, M. J., Costa, A., Whelan, C., Muccio, F., & Henry, K. (2013). Development of an inventory to measure specific phobia of vomiting (Emetophobia). Cognitive Therapy and Research, 37(3), 595-604.
Veale, D., Murphy, P., Ellison, N., Kanakam, N., & Costa, A. (2013). Autobiographical memories of vomiting in people with a specific phobia of vomiting (emetophobia). Journal of behavior therapy and experimental psychiatry, 44(1), 14-20.
Is your fear normal?
Answer our quick surveys below to find out if you have Emetophobia.
